Three Cheers for Three CCC Simulators
Capsulorhexis training devices differ in their similarity to actual surgery. Roibeard Ó hÉineacháin reports

Roibeard O’hEineachain
Published: Tuesday, August 31, 2021
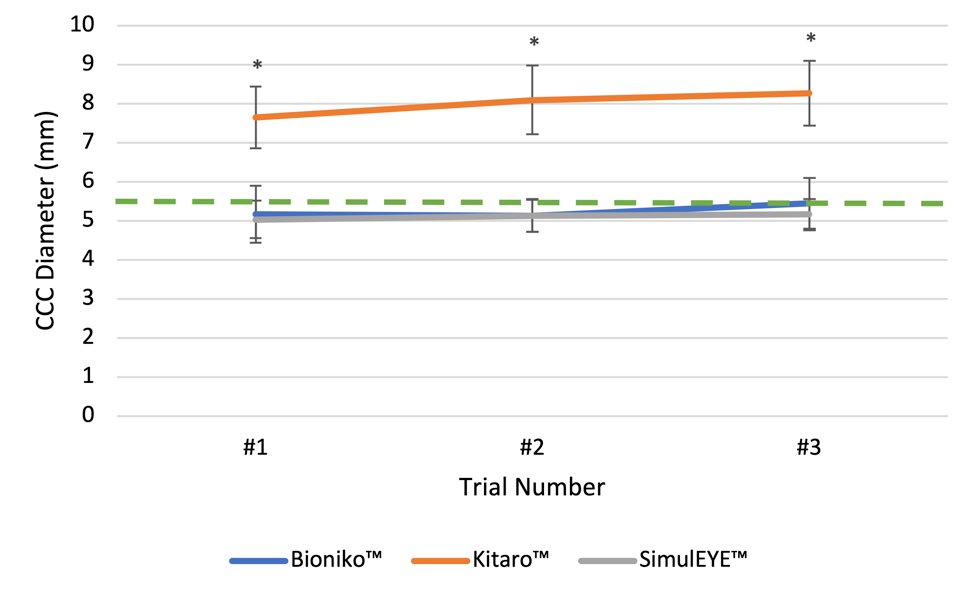 Figure 1: CCC size (mm). Surgeons created the 5.5mm-sized CCC most accurately on Bioniko™ and SimulEYE™. The dashed green line indicates the tasked CCC size of 5.5mm. The CCC on *Kitaro™ was significantly larger than on Bioniko™ and SimulEye™ (p<0.0001) across all trials.
Figure 1: CCC size (mm). Surgeons created the 5.5mm-sized CCC most accurately on Bioniko™ and SimulEYE™. The dashed green line indicates the tasked CCC size of 5.5mm. The CCC on *Kitaro™ was significantly larger than on Bioniko™ and SimulEye™ (p<0.0001) across all trials.
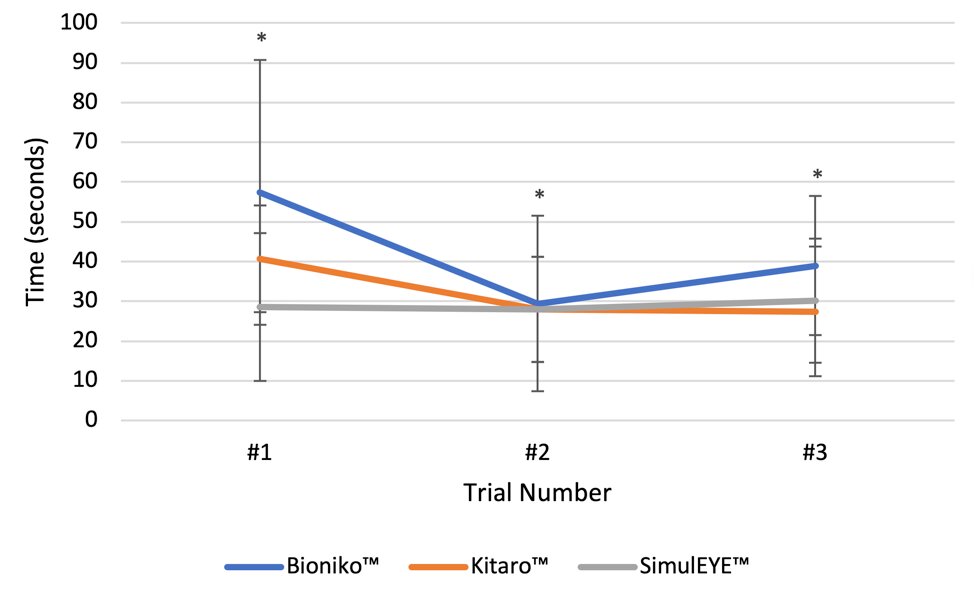 Figure 2: Duration of CCC (seconds). Surgeons took the longest amount of time to perform the CCC on Bioniko™ compared to Kitaro™ (p=0.02) and SimulEYE™ (p=0.002).
Figure 2: Duration of CCC (seconds). Surgeons took the longest amount of time to perform the CCC on Bioniko™ compared to Kitaro™ (p=0.02) and SimulEYE™ (p=0.002).
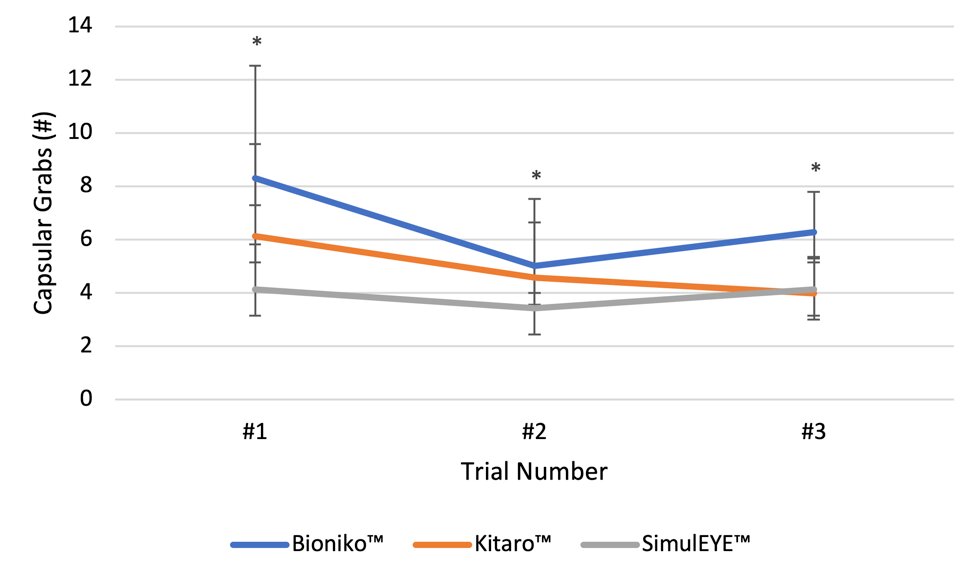 Figure 3: Number of Capsular Grabs: Bioniko™ required a greater number of grabs compared to Kitaro™ p=0.01 and SimulEYE™ (p<0.0001).
Figure 3: Number of Capsular Grabs: Bioniko™ required a greater number of grabs compared to Kitaro™ p=0.01 and SimulEYE™ (p<0.0001).
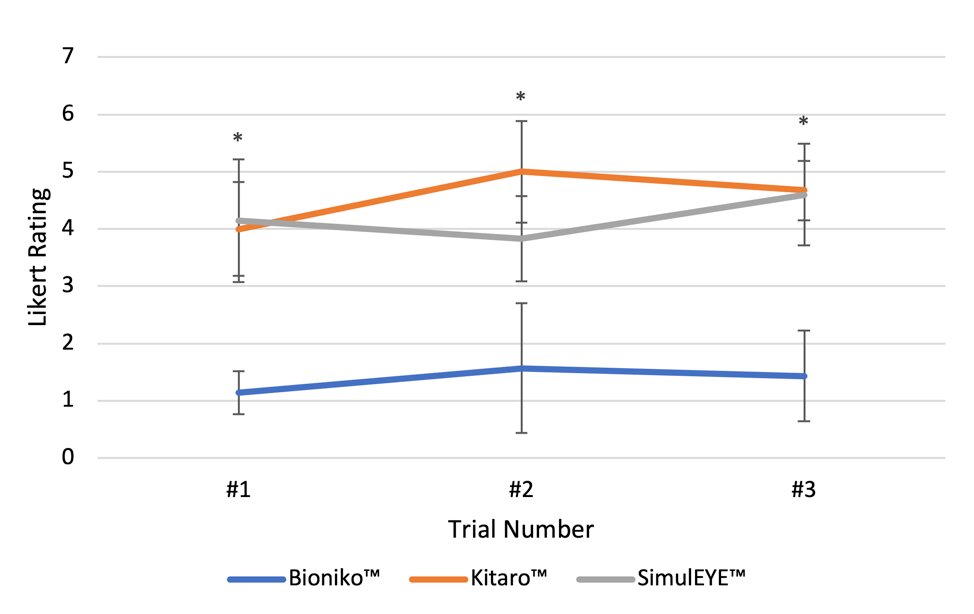 Figure 4: Realism of CCC experience based on modified Likert rating (1-7): Surgeons rated the CCC experience on Kitaro™ and SimulEYE™ as more realistic than on Bioniko™ (p<0.0001).
Figure 4: Realism of CCC experience based on modified Likert rating (1-7): Surgeons rated the CCC experience on Kitaro™ and SimulEYE™ as more realistic than on Bioniko™ (p<0.0001).
Tags: cataract and refractive
Latest Articles
Making Female Leadership More than a Moment
A remarkable global confluence of women in key positions.
ESCRS Talks Technology at AAO
Europe adopts technological advances, US still waiting for lenses and lasers.
Sorting Out Simultaneous Vision IOLs
The ESCRS Eye Journal Club discuss a new landmark paper on IOL classification and the need for harmonisation of terminology for presbyopic IOLs.
Big Advantages to Small-Aperture IOLs
Small-aperture IOLs offer superior image quality with increased range of focus.
Prioritising Self-Care
Benefits of maintaining physical, emotional, and mental health extend beyond the personal sphere.
Valuing Clinical Trial Design
How inclusivity and diversity can enhance scientific accuracy in research.
Knowing Iris Repair: Using Iridodiathermy in Iris Surgery
Prepare for decentred pupils and uneven irides in multiple situations.
Neuroprotectant Treatment for MacTel Type 2
Intravitreal implant releasing ciliary neurotrophic factor found safe and effective in pivotal trials.