Cornea
Knowing Iris Repair: Using Iridodiathermy in Iris Surgery
Prepare for decentred pupils and uneven irides in multiple situations.

Soosan Jacob
Published: Tuesday, April 1, 2025
An uneven iris and a decentred or not round pupil can be addressed in different ways. This article discusses the problems that such situations lead to and what can be done.
Irregular anterior chamber
During pupilloplasty, taking the needle bites too close to the iris edge on either side can cause a gap between two consecutive pupilloplasty knots along a stretch of iris repair. The suture may also sometimes cheese-wire if too close to the edge.
On the other hand, if the needle bites are at a distance from the iris edge, bunching may be seen at the site where the knot tightens to bring the two limbs of iris tissue together. The amount of bunching depends on the distance between the edge and the needle bite—the greater the distance, the greater the bunching.
This bunching can sometimes not be avoided and can lead to the iris tenting upwards locally, causing an asymmetry in the anterior chamber (AC) volume and resulting in an AC that is shallower over the area of pupilloplasty. Though this may not cause problems in most cases, it can become an issue whenever air is to be left in the AC, e.g., post-air injection for a detached Descemet’s membrane (DM) or after endothelial keratoplasty.
The uneven AC can result in an irregular air bubble that is not uniform and may easily migrate partially or completely behind the iris, leading to localized or circumferential iridocorneal touch with an increased risk of peripheral anterior synechiae formation. In such cases, and especially if the eye is also monocameral (e.g., post intrascleral haptic fixation or after iris fixation of IOL), posterior migration of air into the vitreous cavity can occur, resulting in an increased risk of graft detachment.
Floppy iris
Certain eyes may have a floppy iris, which again becomes significant when air bubble dynamics are important. A floppy iris has excess mobility and can result in intra- and postoperative fluctuations in the AC depth, pupillary block, anterior iris bowing, shallow AC, and increased intraocular pressure. A shallow AC can result in difficulty in intraoperative manoeuvring of instruments and damage to ocular structures. This again becomes significant in endothelial keratoplasty, where air is left in the AC to hold the graft up against the host stroma. It also makes it easier for the air to migrate to the posterior chamber or the vitreous cavity in monocameral eyes, resulting in loss of support for the graft.
Decentred, non-circular pupil
The optical and neural axes of the eye are generally well aligned to allow good-quality foveal image formation. The pupil may be found decentred in some patients as a result of previous surgery, trauma, or inflammation, among others. A round and cantered pupil is important for good quality of vision. Prismatic effects can come with a tilted optical system. Decentration of the pupil induces higher-order aberrations and astigmatism, decreased light sensitivity, decreased contrast, changes in refractive error, and distortions in colour, depth, and size perception. When light rays fall obliquely on photoreceptors, each ray may stimulate more than one cone, resulting in acuity loss due to a retinal directional acuity effect. In addition, if performing iris repair, it is important to ensure a well-cantered and round pupil at the end of surgery.
Iridodiathermy
Endodiathermy has been used for many years in vitrectomy surgeries to arrest bleeding, mark the retina around holes or tears, and create retinotomies. More recently, it has been used in iris surgery. A full vitrectomy machine is not required for using the endodiathermy probe, and it can connect to the phaco machine or a cautery unit through its connecting wires. The probe is available as a 23, 25, and 27 gauge and can be inserted through a paracentesis. The effect is activated only at the tip.
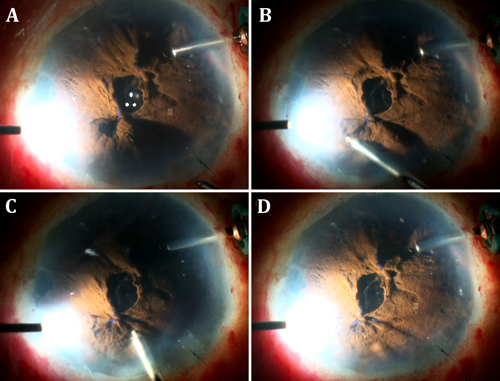
I have described iridodiathermy for treating localized iris bunching adjacent to pupilloplasty knots. The AC is irrigated with BSS via an anterior chamber maintainer. The tip of the endodiathermy probe is applied directly over the bunched-up iris and power activated. This results in contraction of the iris stroma and flattening. The power is kept low and test burns are applied, followed by slow titration upwards until the desired effect is obtained. Spots may be applied until the iris becomes flat and the AC is regular and of even depth again.
A floppy iris is similarly treated by placing spots on the mid-peripheral iris stroma. This causes the iris stroma to contract and tighten, thus tautening the floppiness. Going too close to the pupil should be avoided as this can result in distortion and drawing of the pupil to the side with the spots.
Ahmed (et al.) described the use of endodiathermy for cantering the pupil.1 It may be performed primarily in a case where the pupil is decentred secondary to disease, congenitally, or secondary to surgery/after pupilloplasty. Primary endodiathermal pupillary repositioning is done by simply using the endodiathermy probe. In this case, power is applied close to the pupillary margin and not at the iris, mid-periphery. The iris is drawn towards the endodiathermy application side. It can also be used to round up a non-circular iris using a short application very close to the iris border.
Eyes undergoing penetrating keratoplasty may sometimes need extensive anterior segment reconstruction to improve vision, decrease photic phenomena, release peripheral anterior synechiae, and improve AC dynamics. Suture pupilloplasty is often used to bring iris tissue together into as physiological a position as possible. Open sky endodiathermy can be applied in these cases to flatten the bunched-up iris.
Other uses for the endodiathermy probe in the anterior segment include creating a rhexis or creating a pupil in eyes with an occluded or fully updrawn pupil. The endodiathermy gives a greater effect on a darkly pigmented iris than on light-coloured irides. Also, with time, a mild depigmentation may be seen at the site of application of spots.
This is the seventh article in a series on iris repair. Please see past issues of EuroTimes for related columns.
Dr Soosan Jacob is Director and Chief of Dr Agarwal’s Refractive and Cornea Foundation at Dr Agarwal’s Eye Hospital, Chennai, India, and can be reached at dr_soosanj@hotmail.com.
1. Ahmed I, et al. “Endothermal pupilloplasty to optimize pupil centration, size, and contour,” J Cataract Refract Surg, 2021 Dec 1; 47(12): e80–e83.