Preventing paediatric myopia
With an ever-growing worldwide burden, prevention and correction of myopia are essential.

Soosan Jacob
Published: Thursday, April 1, 2021
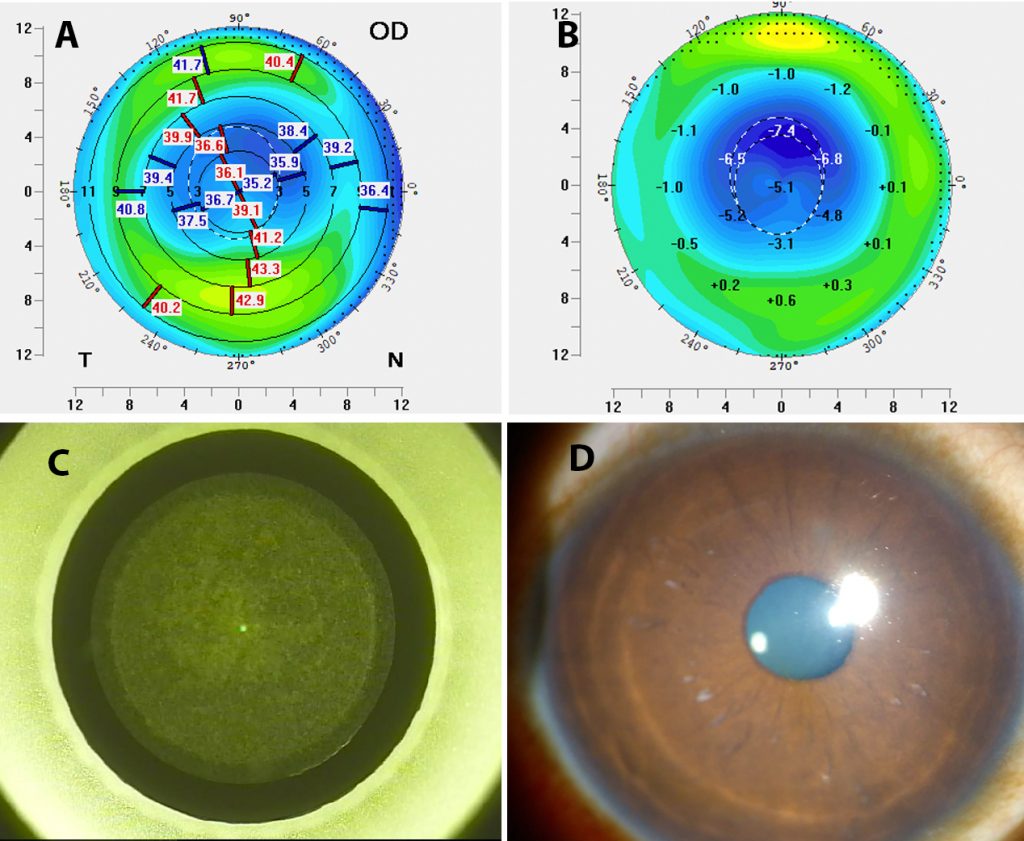 Postoperative topography (A), difference map (B), SMILE corneal cuts (C) and two-year postoperative slit-lamp image (D) showing well-centred correction in a child whose amblyopia reversed after SMILE for myopic anisometropic
A worldwide projected 50% incidence of myopia by 2025 makes this epidemic a serious public health burden. What causes myopisation? An interplay of various genetic and environmental factors that are still not fully understood.
Normally, the emmetropisation process of scleral elongation tries to match the optical axis length to corneal and lenticular power. A feedback mechanism for emmetropisation proposes the afferent sensory arm to be located in the midperipheral, retro-equatorial ocular region. Peripheral defocus stimulates axial elongation and this theory is supported by the axial myopia that is seen after laser photocoagulation of the peripheral retina but not after anti-VEGF therapy in infants with retinopathy of prematurity.
PREVENTION OF MYOPIA
Spectacles and contact lenses:Peripheral light focusing behind the retina (peripheral hyperopic defocus) leads to axial length elongation while an anterior focus (peripheral myopic defocus) slows myopic progression. Conventional myopic single-vision lenses and standard contact lenses cause peripheral hyperopic defocus. Spectacles with progressive addition lenses (PAL), peripheral asphericised PAL, defocus incorporated multiple segments and multifocal/ multifocal-like contact lenses are therefore being tried in children between 8 and 12 years of age to slow myopisation by providing peripheral myopic defocus and decreasing hyperopic blur.
Though benefit has been shown in decreasing axial length elongation and myopia progression, the optimum amount of add power required, hours of use per day, number of years of treatment required and the permanency of effect once lens wear is stopped are all questions still needing answers.
Orthokeratology or ortho-k uses rigid contact lenses worn overnight to flatten the cornea while sleeping, thus decreasing the need for corrective lenses during daytime. The oblate change in corneal shape may also slow myopia progression by keeping the macular image in focus while providing a myopic peripheral defocus.
Topical Atropine: The mechanism of action though yet unknown is not related to accommodation. Low-dose Atropine at 0.01% has been used in children from 5 to 17 years of age to decrease myopia progression. It is better tolerated than higher doses while not differing significantly in efficacy and having less myopic rebound on cessation. Poor responders may be given a stepwise increase in dose. The effect is seen to have geographical variation and ideal concentration and dosing are still being evaluated with more region-specific studies required. Rebound myopia on cessation may be decreased by using lower doses, tapering dose once stable and continuing treatment till more than 12 years age or into late teens.
Other anti-muscarinics as well as dopamine, a major neurotransmitter in the retina are also being studied. Dopamine and/or other unidentified molecules may act as messengers that transfer information from the afferent to the efferent arm of the feedback mechanism for emmetropisation.
Vision training: Accommodative abnormalities seen in myopic patients can cause retinal image degradation and increasing myopia, e.g., an increased lag of accommodation may be myopigenic. Patients on PAL adapt with time and redevelop accommodation lag. In addition, PAL may cause degradation of extrafoveal image due to inherent design and may also cause myopia at near.
Vision training for accommodation may therefore be important. Custom soft contact lenses are being studied to alter spherical aberration, improve accommodation and reduce accommodation lag. The CAMS study tried to improve accommodative accuracy and dynamics using vision training and alteration of spherical aberration.
Lifestyle modifications: Environmental factors including outdoor time, prolonged and intense periods of close work, urbanisation etc have been associated with myopia progression and a multi-pronged approach to prevention gives additive effects.
SURGICAL CORRECTION FOR MYOPIA
Children with unilateral or bilateral high myopia with failed conventional therapy with glasses and contact lenses may need surgery. The question, however, still remains as to the threshold level for refractive surgery. Dr Paysee, at the 3rd World Congress of Paediatric Ophthalmology and Strabismus, Barcelona, suggested ≥4.0D for severe anisometropia and ≥-6.0D for severe isoametropia, though in practice, patients who have failed with glasses and contact lenses tend to have much higher values. Surgery is also beneficial in children unable to wear glasses or contact lenses due to altered facial or ocular anatomy, neurobehavioural or developmental problems, intellectual disabilities etc.
Advantages of surgical correction are many and include improved refraction, vision and stereopsis as also more effective amblyopia therapy less dependent on patient and parental compliance, full-time visual correction, social and psychological improvement and a more alert and involved child.
Challenges are also many and include those of a growing eye, changing refractive status, difficult pre- and postoperative assessment, difficult surgery and difficult recognition and management of postoperative complications. Surgery is generally preferred after 2 years of age because of the large changes with growth in the first two years.
The major indication for surgery is anisometropic amblyopia. As in all paediatric refractive surgeries, the target refractive correction opted for needs to be decided at the time of surgery. The aim should be to bring the refraction to a point where the child can function visually and amblyopia can be prevented. Perfection may not always be necessary as in adults. The need for follow-up amblyopia therapy cannot be under-stressed.
Laser vision correction (LVC): Surface ablation is often preferred in children, because of absent risk for flap-related complications that may occur post-LASIK. Postoperative steroids are important to avoid haze and regression. LASIK may be performed but flap-related complications are an ever-present threat in children. A more recent option is small-incision lenticule extraction (SMILE ®), which avoids many of the risks of LASIK and surface ablation while giving good predictability, efficacy and stability. SMILE is not affected by anaesthetic gases unlike excimer laser.
Irreversibility, the need for patient cooperation for centration, inability to fixate under anaesthesia, risk for decentred ablation and induction of aberrations are challenges associated with all LVC techniques. The need for an anaesthesia machine is also a challenge as most refractive suites don’t have the facility.
INTRAOCULAR SURGERY
An untouched cornea, less aberration induction and better retinal image magnification in extreme myopias nearing -20D are advantages of phakic IOLs (PIOLs) and refractive lens exchange (RLE). However, the risk of complications such as retinal tears and detachment secondary to intraocular surgery in such high myopic eyes needs to be kept in mind and thorough pre- and postoperative retinal examinations are a must.
PIOLs: Lesueur et al showed good safety, refractive and functional outcomes and improvement in quality of life with posterior chamber PIOLs (Visian ICL, Staar Surgical) for paediatric high myopia at the 2017 WSPOS Paediatric Subspecialty Day meeting. Advantages include small incision and reversibility. Cataractogenesis is reported to be less frequent with the V4c model. Silicone PIOLs have been reported to be associated with vitreous luxation of the IOL either due to intra-operative manipulation or cheese-wiring of zonular fibres.
The ideal age for surgery with PIOLs is controversial, since optimum sizing of the ICL and thereby the vault changes with growth of the eye. Though anterior chamber PIOLs may also be used, long term endothelial concerns have traditionally limited their use in the paediatric population.
RLE: This may be indicated for children with refractive errors exceeding -20D and with insufficient anterior chamber depth. Standard cataract techniques recommended as per the age of the child are used. The loss of accommodation and increased inflammatory response together with the increased risk for glaucoma and posterior segment complications are the biggest disadvantages of RLE. Multifocal and EDOF IOLs are being tried in children but conclusive results are yet awaited.
Bioptics: Sequential refractive surgeries may be employed for very high refractive errors. For example, PIOL may be followed up with LASIK for any residual refractive error needing correction or for any new refractive error developing with growth of the eye. Treatment may be done after 18 years of age once refraction is stabilised.
Dr Soosan Jacob is Director and Chief of Dr Agarwal’s Refractive and Cornea Foundation at Dr Agarwal’s Eye Hospital, Chennai, India and can be reached at dr_soosanj@hotmail.com
Postoperative topography (A), difference map (B), SMILE corneal cuts (C) and two-year postoperative slit-lamp image (D) showing well-centred correction in a child whose amblyopia reversed after SMILE for myopic anisometropic
A worldwide projected 50% incidence of myopia by 2025 makes this epidemic a serious public health burden. What causes myopisation? An interplay of various genetic and environmental factors that are still not fully understood.
Normally, the emmetropisation process of scleral elongation tries to match the optical axis length to corneal and lenticular power. A feedback mechanism for emmetropisation proposes the afferent sensory arm to be located in the midperipheral, retro-equatorial ocular region. Peripheral defocus stimulates axial elongation and this theory is supported by the axial myopia that is seen after laser photocoagulation of the peripheral retina but not after anti-VEGF therapy in infants with retinopathy of prematurity.
PREVENTION OF MYOPIA
Spectacles and contact lenses:Peripheral light focusing behind the retina (peripheral hyperopic defocus) leads to axial length elongation while an anterior focus (peripheral myopic defocus) slows myopic progression. Conventional myopic single-vision lenses and standard contact lenses cause peripheral hyperopic defocus. Spectacles with progressive addition lenses (PAL), peripheral asphericised PAL, defocus incorporated multiple segments and multifocal/ multifocal-like contact lenses are therefore being tried in children between 8 and 12 years of age to slow myopisation by providing peripheral myopic defocus and decreasing hyperopic blur.
Though benefit has been shown in decreasing axial length elongation and myopia progression, the optimum amount of add power required, hours of use per day, number of years of treatment required and the permanency of effect once lens wear is stopped are all questions still needing answers.
Orthokeratology or ortho-k uses rigid contact lenses worn overnight to flatten the cornea while sleeping, thus decreasing the need for corrective lenses during daytime. The oblate change in corneal shape may also slow myopia progression by keeping the macular image in focus while providing a myopic peripheral defocus.
Topical Atropine: The mechanism of action though yet unknown is not related to accommodation. Low-dose Atropine at 0.01% has been used in children from 5 to 17 years of age to decrease myopia progression. It is better tolerated than higher doses while not differing significantly in efficacy and having less myopic rebound on cessation. Poor responders may be given a stepwise increase in dose. The effect is seen to have geographical variation and ideal concentration and dosing are still being evaluated with more region-specific studies required. Rebound myopia on cessation may be decreased by using lower doses, tapering dose once stable and continuing treatment till more than 12 years age or into late teens.
Other anti-muscarinics as well as dopamine, a major neurotransmitter in the retina are also being studied. Dopamine and/or other unidentified molecules may act as messengers that transfer information from the afferent to the efferent arm of the feedback mechanism for emmetropisation.
Vision training: Accommodative abnormalities seen in myopic patients can cause retinal image degradation and increasing myopia, e.g., an increased lag of accommodation may be myopigenic. Patients on PAL adapt with time and redevelop accommodation lag. In addition, PAL may cause degradation of extrafoveal image due to inherent design and may also cause myopia at near.
Vision training for accommodation may therefore be important. Custom soft contact lenses are being studied to alter spherical aberration, improve accommodation and reduce accommodation lag. The CAMS study tried to improve accommodative accuracy and dynamics using vision training and alteration of spherical aberration.
Lifestyle modifications: Environmental factors including outdoor time, prolonged and intense periods of close work, urbanisation etc have been associated with myopia progression and a multi-pronged approach to prevention gives additive effects.
SURGICAL CORRECTION FOR MYOPIA
Children with unilateral or bilateral high myopia with failed conventional therapy with glasses and contact lenses may need surgery. The question, however, still remains as to the threshold level for refractive surgery. Dr Paysee, at the 3rd World Congress of Paediatric Ophthalmology and Strabismus, Barcelona, suggested ≥4.0D for severe anisometropia and ≥-6.0D for severe isoametropia, though in practice, patients who have failed with glasses and contact lenses tend to have much higher values. Surgery is also beneficial in children unable to wear glasses or contact lenses due to altered facial or ocular anatomy, neurobehavioural or developmental problems, intellectual disabilities etc.
Advantages of surgical correction are many and include improved refraction, vision and stereopsis as also more effective amblyopia therapy less dependent on patient and parental compliance, full-time visual correction, social and psychological improvement and a more alert and involved child.
Challenges are also many and include those of a growing eye, changing refractive status, difficult pre- and postoperative assessment, difficult surgery and difficult recognition and management of postoperative complications. Surgery is generally preferred after 2 years of age because of the large changes with growth in the first two years.
The major indication for surgery is anisometropic amblyopia. As in all paediatric refractive surgeries, the target refractive correction opted for needs to be decided at the time of surgery. The aim should be to bring the refraction to a point where the child can function visually and amblyopia can be prevented. Perfection may not always be necessary as in adults. The need for follow-up amblyopia therapy cannot be under-stressed.
Laser vision correction (LVC): Surface ablation is often preferred in children, because of absent risk for flap-related complications that may occur post-LASIK. Postoperative steroids are important to avoid haze and regression. LASIK may be performed but flap-related complications are an ever-present threat in children. A more recent option is small-incision lenticule extraction (SMILE ®), which avoids many of the risks of LASIK and surface ablation while giving good predictability, efficacy and stability. SMILE is not affected by anaesthetic gases unlike excimer laser.
Irreversibility, the need for patient cooperation for centration, inability to fixate under anaesthesia, risk for decentred ablation and induction of aberrations are challenges associated with all LVC techniques. The need for an anaesthesia machine is also a challenge as most refractive suites don’t have the facility.
INTRAOCULAR SURGERY
An untouched cornea, less aberration induction and better retinal image magnification in extreme myopias nearing -20D are advantages of phakic IOLs (PIOLs) and refractive lens exchange (RLE). However, the risk of complications such as retinal tears and detachment secondary to intraocular surgery in such high myopic eyes needs to be kept in mind and thorough pre- and postoperative retinal examinations are a must.
PIOLs: Lesueur et al showed good safety, refractive and functional outcomes and improvement in quality of life with posterior chamber PIOLs (Visian ICL, Staar Surgical) for paediatric high myopia at the 2017 WSPOS Paediatric Subspecialty Day meeting. Advantages include small incision and reversibility. Cataractogenesis is reported to be less frequent with the V4c model. Silicone PIOLs have been reported to be associated with vitreous luxation of the IOL either due to intra-operative manipulation or cheese-wiring of zonular fibres.
The ideal age for surgery with PIOLs is controversial, since optimum sizing of the ICL and thereby the vault changes with growth of the eye. Though anterior chamber PIOLs may also be used, long term endothelial concerns have traditionally limited their use in the paediatric population.
RLE: This may be indicated for children with refractive errors exceeding -20D and with insufficient anterior chamber depth. Standard cataract techniques recommended as per the age of the child are used. The loss of accommodation and increased inflammatory response together with the increased risk for glaucoma and posterior segment complications are the biggest disadvantages of RLE. Multifocal and EDOF IOLs are being tried in children but conclusive results are yet awaited.
Bioptics: Sequential refractive surgeries may be employed for very high refractive errors. For example, PIOL may be followed up with LASIK for any residual refractive error needing correction or for any new refractive error developing with growth of the eye. Treatment may be done after 18 years of age once refraction is stabilised.
Dr Soosan Jacob is Director and Chief of Dr Agarwal’s Refractive and Cornea Foundation at Dr Agarwal’s Eye Hospital, Chennai, India and can be reached at dr_soosanj@hotmail.com
Tags: paediatric myopia
Latest Articles
Towards a Unified IOL Classification
The new IOL functional classification needs a strong and unified effort from surgeons, societies, and industry.
Organising for Success
Professional and personal goals drive practice ownership and operational choices.
Update on Astigmatism Analysis
Is Frugal Innovation Possible in Ophthalmology?
Improving access through financially and environmentally sustainable innovation.
iNovation Innovators Den Boosts Eye Care Pioneers
New ideas and industry, colleague, and funding contacts among the benefits.
José Güell: Trends in Cornea Treatment
Endothelial damage, cellular treatments, human tissue, and infections are key concerns on the horizon.
Making IOLs a More Personal Choice
Surgeons may prefer some IOLs for their patients, but what about for themselves?
Need to Know: Higher-Order Aberrations and Polynomials
This first instalment in a tutorial series will discuss more on the measurement and clinical implications of HOAs.
Never Go In Blind
Novel ophthalmic block simulator promises higher rates of confidence and competence in trainees.