IOL
Capsular Bag or Sulcus?
Which is better for accommodating IOLs? Fixation site may influence longevity of action, risk of complications. Howard Larkin reports from Milan.

Howard Larkin
Published: Wednesday, November 9, 2022
Accommodating intraocular lenses (AIOLs) are the ultimate goal for treating presbyopia and cataract. As AIOLs are developed, whether it’s better to fixate them in the capsular bag or the sulcus has emerged as a significant design question.
The answer turns on the durability and reliability of any mechanism of action between the two locations and whether one may be more prone to inflammation or other complications than the other. Eric Donnenfeld MD and Jorge L Alió MD, PhD debated the relative merits of each option in the Journal of Cataract and Refractive Surgery symposium at the 40th Congress of the ESCRS in Milan.
IN THE BAG
Arguing for capsular bag fixation, Dr Donnenfeld pointed out the bag is avascular, stable, reproducible, and non-inflammatory. However, he noted the lessons learned from previous failed attempts at in-the-bag AIOLs.
The Crystalens® (Bausch + Lomb) relied on capsular bag contraction to move its single optic back and forth on hinged haptics. But fibrosis quickly reduced its ability to contract and potentially move the lens, also leading to decentration and tilt, Dr Donnenfeld said.
The Visiogen Synchrony showed that by filling the capsular bag, posterior capsule opacification (PCO) and fibrosis could be greatly reduced. But its dual optic design required moving the lenses to accommodate, which turned out to be more difficult than changing the curvature of a fluid-filled optic, he said.
Newer, fluid-filled ACIOL designs prevent capsular bag opacification by limiting contact between the anterior capsule and the anterior optic surface and maintaining an open and expanded capsular bag. These include the Gemini Refractive Capsule (Omega Ophthalmics), PowerVision (Alcon), and Juvene (LensGen) modular lenses.
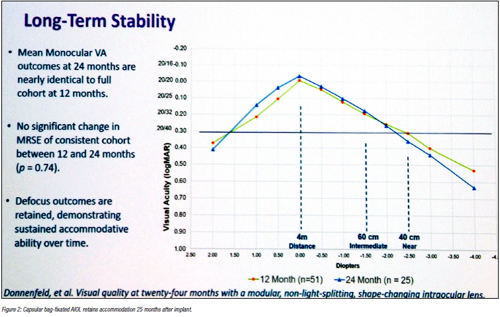
“The capsule remains clear, it remains pliable, and five-year clinical data supports PCO prevention, refractive, and long-term accommodation stability. Capsular fibrosis and opacification are not unavoidable,” Dr Donnenfeld said. He noted the Juvene IOL, which he has helped test, provided binocular visual acuity of better than 20/40 from +2.00 D to -2.50 D—and maintained this range up to two years after surgery, though long-term efficacy is unknown.
The capsular bag is also easy to access for surgeons, Dr Donnenfeld added. By contrast, the sulcus is very tight, crowded by the iris, ciliary processes, and choroid. And unlike the capsular bag, these tissues are highly vascular, metabolically active, and subject to inflammatory responses. Known complications of sulcus fixation include chronic tissue irritation, anterior uveitis, iridocyclitis, and iris chaffing.
The sulcus is also rigid with variable anatomy making sizing critical, and visualisation is difficult, Dr Donnenfeld added. “Putting a lens there is like putting it between a rock and a hard place,” he said. “The question is not whether Jorge Alió can implant a haptic in the sulcus without visualisation, but whether the average surgeon can.”
IN THE SULCUS
Arguing for sulcus fixation of AIOLs, Dr Alió noted the capsular bag is the basal membrane of the lens epithelium—and once the lens tissue is removed, it has no anatomical reason to exist, making fibrosis and atrophy inevitable. He has demonstrated this in a primate model, in which a measuring device implanted in the capsular bag to detect the forces of the ciliary body continued to generate contractile force in the sulcus, but not in the capsular bag six months after lens removal. There was also no inflammation due to the sulcus-fixated haptics for five years after implant.i–ii
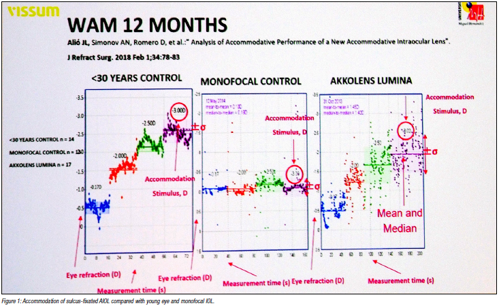
Dr Alió has extensively tested the AkkoLens Lumina, a sulcusfixated AIOL that accommodates by sliding two optics across each other in response to ciliary contraction. It objectively shows accommodation under stimuli of up to -3.00 D. Contract sensitivity is also like a monofocal lens.
The Lumina AIOL also showed objective accommodation of about two-thirds the magnitude of a 30-year-old control patient 1 year after surgery.iii Current studies show a stable accommodative outcome out to 3.3 years after surgery, Dr Alió said. Refraction also remained stable across all distances after YAG capsulotomy, and the lens can be implanted even after a posterior capsule break. In addition, the Lumina provided better quality of vision compared to an extended depth of focus IOL.
Dr Alió pointed out the Lumina is the only AIOL with highly rated published evidence, demonstrating that a sulcus-fixated AIOL is viable.iv
He concluded accommodative IOLs are monofocal lenses that change in power according to distance. This concept completely differs from monofocality, he said, which involves an overlap of images requiring neuroadaptation—something that does not happen in real accommodative lenses.
“Once AIOLs are developed adequately, multifocal IOLs will be unable to compete, as happened with pseudophakic glasses and monofocal lenses of the first generation.”
i Alió JL, Ben-Nun J. Journal of Refractive Surgery. 2015; 31: 124–128.
ii Alió JL, Ben-Nun J. Journal of Refractive Surgery. 2005; 31: 1802–1808.
iii Alió JL et al. American Journal of Ophthalmology. 2016 Jan 29. doi: 10.1016/j.ajo.2016.01.006.
iv Alió JL et al. American Journal of Ophthalmology. 2016 Apr; 164: 37–48.
Eric D Donnenfeld MD is clinical professor of ophthalmology at New York University in New York City, US; trustee of Dartmouth Medical School in Hanover, New Hampshire, US; and in private practice in New York State, US. ericdonnenfeld@gmail.com
Jorge L Alió MD, PhD is professor and the chairman of ophthalmology at Miguel Hernández University of Elche and scientific director at Vissum in Alicante, Spain. jlalio@vissum.com