Preparation is key in tackling PCR during cataract surgery
Dermot McGrath
Published: Monday, February 1, 2021
Sharp edge to capsular break
Adequate preparation and a clear strategy can help surgeons to deal successfully with posterior capsule rupture (PCR) when it occurs during cataract surgery, according to Richard Packard MD, FRCS, FRCOphth.
“It is important to have a strategy in place and not to panic. Denial at its most basic is saying something hasn’t happened, which means denying a painful reality. We need to be able to recognise trouble early and get over the denial that the posterior capsule is really gone. We generally do not lose vitreous and we usually know where it has gone but just don’t like to admit it,” he said at the 38th Congress of the ESCRS.
Mr Packard, Senior Consultant at Arnott Eye Associates, London, United Kingdom, said it was important to remember that a broken capsule during phacoemulsification does not necessarily equate to vitreous loss. “We need to check the edge of the break for vitreous prolapse. If it is sharp, it means that the anterior hyaloid has not been breached. However, if there is a scalloped edge there is vitreous prolapsing and we need to plan accordingly,” he said.
Scalloped edge to capsular break
Once a rupture has been identified, it is critical not to allow the eye to decompress, as this will allow vitreous to prolapse, advised Mr Packard.
“Fill the eye with a dispersive ophthalmic viscosurgical device (OVD) before removing the phaco probe. It is important to maintain irrigation while the dispersive viscoelastic is being injected to tamponade the break. At this point, the anterior hyaloid has not been breached so it is perfectly feasible to fill the eye and get things stable so that you can make a plan to rescue the situation,” he said.
In 2000 it was shown that triamcinalone could allow vitreous to be made visible. This has transformed the way that it is dealt with.
Should an anterior vitrectomy be required, it is advisable to have an emergency kit available that contains all the required tools for the task in hand, said Mr Packard.
The kit should include a vitrector set up for bimanual use with a trocar, dispersive OVD, triamcinolone for intracameral use, Miochol for pupil constriction, a Sheets glide, a vectis, and 10/0 nylon suture and needle holder. An appropriate lens for the post-vitrectomy eye should also be available. As already stated, injecting triamcinolone will help the surgeon to uncloak the vitreous and facilitate vitreous clean-up in cases of PCR.
CORNEAL OR PARS PLANA INCISIONS
The next step is to decide if the vitrectomy will be performed through corneal or pars plana incisions, said Mr Packard.
“Whether you go through the pars plana or not will to some extent depend on the size of your vitrectomy cutter: 25-gauge will be pars plana, 23-gauge could be either corneal or pars plana, and 20-gauge will be the corneal route,” he said.
Although pars plana is more efficient, Mr Packard said the surgeon should proceed with this technique only if they are prepared to check for and able to deal with peripheral retinal breaks.
“Otherwise, use the corneal entry point. In any event, postoperatively a check for peripheral retinal breaks should be carried out,” he said.
Once the eye has been filled with dispersive OVD, the surgeon needs to ensure a second paracentesis for bimanual vitrectomy. “Do not use the main wound or coaxial vitrectomy as it will just bring more vitreous forward and it’s very inefficient. It will also put stress on the vitreous base,” he said.
For trocar insertion, Mr Packard advised advancing the trocar about 1.5 mm obliquely, then changing the direction of the trocar to 90 degrees towards the posterior pole before pushing inwards.
“Then with a pair of forceps, withdraw the trocar and leave the opening in place. It is important to see that it deviates at an angle because this means you have created a tunnel which is less likely to leak when you remove the trocar,” he said.
Options to remove any nuclear fragments include using dispersive OVD or a Sheets glide to prevent pieces dislocating into the vitreous cavity, or an IOL scaffold approach using a three-piece IOL as a barrier to compartmentalise the anterior and posterior chambers and enable phacoemulsification of the remaining fragments.
Mr Packard recommended clearing central vitreous first using cut/irrigation-aspiration settings and injecting triamcinolone as required to check for residual vitreous.
Residual vitreous exposed
“A key word of advice here is not to use a sponge to pull on the vitreous wick because that will put stress on the vitreous base and is more likely to lead to breaks in the retina. It is important to clear the wound so that the vitrector can then cut away the vitreous,” he said.The choice of IOL will depend on the status of the capsule, said Mr Packard.
“In the event of a small capsular tear with a continuous edge, a one-piece lens may be placed in the capsular bag. If you have got a good rhexis edge with a large posterior capsule tear, then sulcus fixation and optic capture is the best approach. If capsular support is inadequate, then consider an Artisan IOL or the Yamane technique. One can even use a suitably sized anterior chamber IOL in older patients as it can give a reasonable result,” he said.

 Sharp edge to capsular break
Sharp edge to capsular break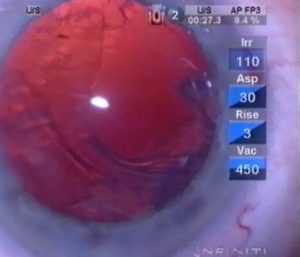 Scalloped edge to capsular break
Scalloped edge to capsular break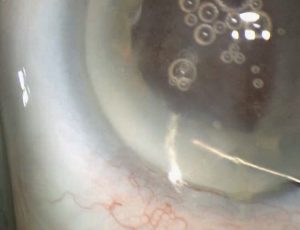 Residual vitreous exposed
Residual vitreous exposed