Myopic foveoschisis
Early intervention correlates with better functional outcome

Cheryl Guttman Krader
Published: Friday, March 1, 2019
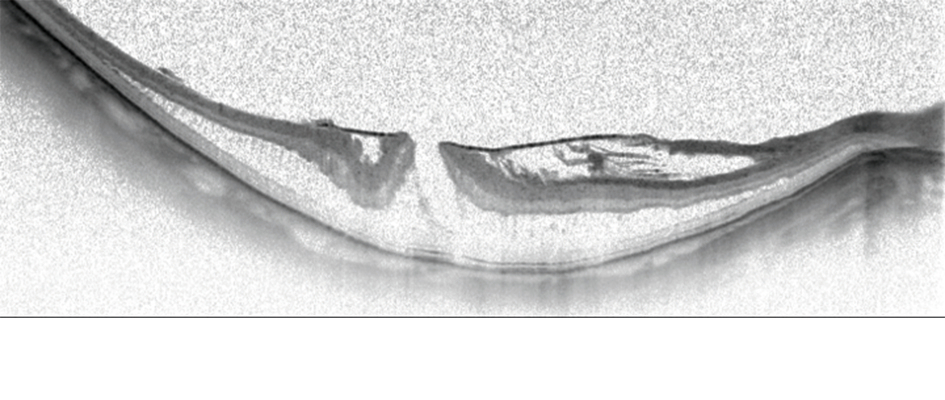 Horizontal OCT scan of a myopic foveoschisis with a premacular membrane[/caption]
Preoperative visual acuity is the main factor influencing functional outcomes after vitrectomy for myopic foveoschisis. With this information in mind, retina specialists aiming to improve their results should consider operating sooner rather than later, said Ramin Tadayoni MD, PhD, at the 18th EURETINA Congress in Vienna, Austria.
“Of course, we can also do better for our patients by using modern surgical techniques and imaging technologies. But, we will have better results if the indication for surgery is good. If the goal is to achieve BCVA [best-corrected visual acuity] better than 20/40, then surgery should be done when the vision is 20/50 or better. We should not wait for the vision to get worse,” said Dr Tadayoni, Professor of Ophthalmology, Paris 7 University, Lariboisière Hospital & OphtalmoPôle, Paris, France.
Horizontal OCT scan of a myopic foveoschisis with a premacular membrane[/caption]
Preoperative visual acuity is the main factor influencing functional outcomes after vitrectomy for myopic foveoschisis. With this information in mind, retina specialists aiming to improve their results should consider operating sooner rather than later, said Ramin Tadayoni MD, PhD, at the 18th EURETINA Congress in Vienna, Austria.
“Of course, we can also do better for our patients by using modern surgical techniques and imaging technologies. But, we will have better results if the indication for surgery is good. If the goal is to achieve BCVA [best-corrected visual acuity] better than 20/40, then surgery should be done when the vision is 20/50 or better. We should not wait for the vision to get worse,” said Dr Tadayoni, Professor of Ophthalmology, Paris 7 University, Lariboisière Hospital & OphtalmoPôle, Paris, France.
 Ramin Tadayoni MD, PhD
Ramin Tadayoni MD, PhD